





Esophageal Cancer
Esophageal cancer is a serious condition that develops in the lining of the esophagus and can progress rapidly if not identified and managed early. It often presents with symptoms like difficulty swallowing (dysphagia), unexplained weight loss, or persistent chest discomfort. Early diagnosis plays a crucial role in improving outcomes.
Esophageal cancer originates in the inner mucosal layer of the esophagus and, if left unchecked, can infiltrate deeper tissues and metastasize. Most patients report progressive dysphagia or significant weight loss. The earlier we diagnose, the more effective the intervention.Treatment usually involves a combination of surgery, chemotherapy, and radiation, depending on the stage of the disease and the patient’s overall health. Surgical intervention may range from traditional open procedures to minimally invasive techniques, which can offer faster recovery and fewer complications.
Types of esophageal cancer Treated by Dr. Harish Ravoori
Adenocarcinoma
Typically arises in the distal esophagus and is often associated with Barrett’s esophagus or chronic gastroesophageal reflux disease (GERD).

Squamous Cell Carcinoma
Generally affects the proximal or mid-esophageal region and is linked to tobacco use, alcohol consumption, and dietary carcinogens.
Treatment Options for Esophageal Cancer
Surgical Treatments: Types of Esophageal Cancer Surgery
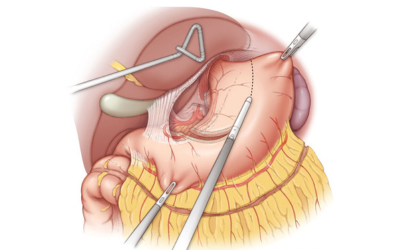
Minimally Invasive Esophagectomy
Performed via laparoscopic and thoracoscopic access, MIE reduces post-operative pain, minimizes scarring, and shortens recovery time while preserving oncologic safety.
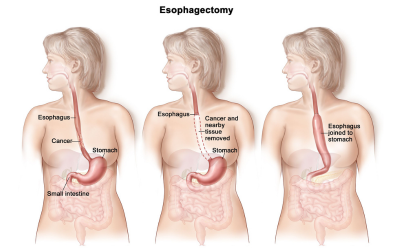
Open Esophagectomy
A traditional approach for locally advanced tumors requiring extensive resection and lymphadenectomy, particularly where minimally invasive access is contraindicated.
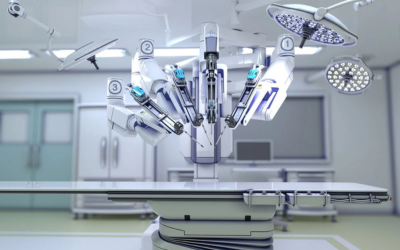
Robotic-assisted Surgery
Robotic systems enhance dexterity, visualization, and surgical precision in complex esophagectomy cases, especially for tumors near vital structures.
Non-Surgical Treatments
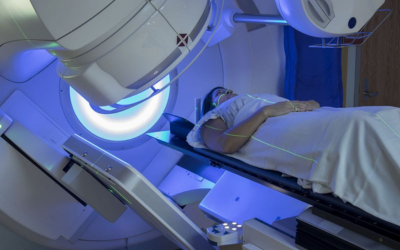
Radiation Therapy
Administers ionizing radiation to destroy cancer cells, often in conjunction with chemotherapy (chemoradiation) to enhance tumor response and control.

Chemotherapy
Utilizes cytotoxic agents to reduce tumor burden, often as neoadjuvant (pre-surgical) or adjuvant (post-surgical) therapy, and in metastatic settings.

Targeted Therapy & Immunotherapy
Advanced agents such as HER2 inhibitors and immune checkpoint inhibitors (e.g., PD-1/PD-L1 blockers) are utilized based on tumor profiling and biomarker expression.

Palliative Care for Advanced Cases
For stage IV or non-operable disease, palliative measures—including stent placement, analgesia, and nutritional support—prioritize symptom relief and dignity in care.
Frequently asked questions
Success rates are highest when diagnosed in early stages. When treated promptly with multimodal care, many patients achieve significant disease control or remission.
Patients typically stay hospitalized for 7–10 days post-surgery, with full recovery spanning 4–8 weeks depending on the surgical method and individual response.
Yes, especially in non-resectable or early-stage tumors. Definitive chemoradiotherapy and systemic therapies offer effective alternatives in select patients.
Stage IV indicates metastatic spread to distant organs (lungs, liver, etc.). In such cases, palliative interventions are prioritized to relieve symptoms and enhance comfort.