




Urological Cancer Treatment
Urological cancers refer to a range of malignancies affecting the urinary and male reproductive systems — including the kidneys, bladder, prostate, testicles, and urethra. These cancers often begin silently, showing little or no symptoms in their early stages.
Many patients seek help only after experiencing warning signs such as blood in urine, frequent or painful urination, or pain in the back or lower abdomen. That’s why early diagnosis and timely treatment play a crucial role in improving recovery and long-term survival.
Types of Urological Cancer Treated by Dr. Harish Ravoori
Let’s look at the major types of urological cancers that Dr. Harish treats with precision and advanced care.
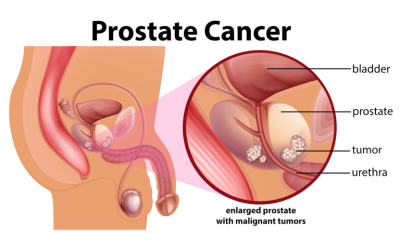
Prostate Cancer
A common cancer in men, prostate cancer often grows slowly but can spread if untreated. Dr. Harish uses minimally invasive or robotic techniques to remove the affected gland while preserving urinary control and sexual function as much as possible.
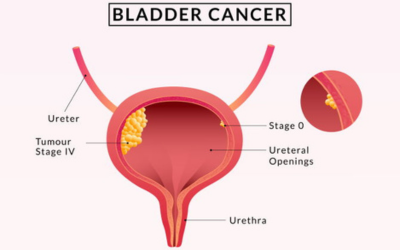
Bladder Cancer
It typically begins in the bladder’s inner lining and may present with blood in urine or frequent urination. Depending on the stage, treatments can include transurethral resection, partial or radical cystectomy, and reconstructive bladder surgery.
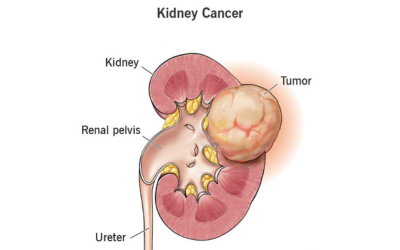
Kidney (Renal) Cancer
Detected increasingly through imaging, kidney cancer is treated by removing only the tumor (partial nephrectomy) or the entire kidney (radical nephrectomy). Minimally invasive and robotic surgeries allow precise tumor removal while preserving kidney function.
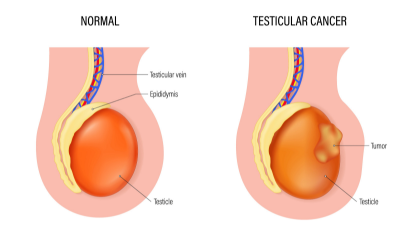
Testicular Cancer
Most common in younger men, testicular cancer is highly curable with prompt treatment. Surgery involves removing the affected testis (orchidectomy) and, in advanced cases, lymph node dissection for accurate staging and cure.
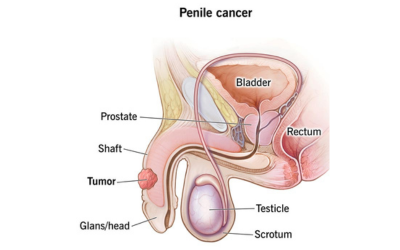
Urethral and Penile Cancer
These are rare but require expert surgical intervention and reconstructive care to maintain urinary and sexual function, which Dr. Harish’s experience and multidisciplinary approach make possible.
Treatment Options for Urological Cancer

Surgery
Surgery is often the first line of treatment for most urological cancers. Using laparoscopic or robotic-assisted methods, Dr. Harish removes the tumor precisely while preserving as much healthy organ tissue as possible, ensuring minimal damage to surrounding structures and faster recovery.

Chemotherapy
Chemotherapy uses anti-cancer drugs to destroy cancer cells or stop their growth. It may be given before surgery to shrink tumors or after to prevent recurrence, especially in bladder and testicular cancers.

Radiotherapy
Radiotherapy directs controlled doses of radiation to the tumor site. It helps eliminate remaining cancer cells after surgery or serves as a primary treatment in cases where surgery isn’t suitable.

Immunotherapy
Immunotherapy boosts the body’s immune system to recognize and attack cancer cells. This newer treatment has shown promising results in certain kidney and bladder cancers with specific biomarkers.

Hormone Therapy
Some cancers, like prostate cancer, grow in response to male hormones. Hormone therapy blocks or reduces these hormones, slowing cancer progression and easing related symptoms.

Targeted Therapy
Targeted therapy focuses on blocking specific molecules that help cancer cells grow. It’s often used in advanced kidney or bladder cancers, offering effective control with fewer side effects.

Combination Therapy
Many patients benefit from a combination of treatments. Surgery, radiation, and drug-based therapies may be used together to increase effectiveness and reduce the risk of recurrence.
Frequently asked questions
Symptoms may include blood in urine, frequent or painful urination, flank pain, unexplained weight loss, or swelling in the testicles. Early evaluation is crucial.
Yes. When diagnosed early and treated by experienced specialists, many urological cancers can be completely cured with surgery and adjunct treatments.
Robotic surgery enhances surgical precision, reduces recovery time, and helps preserve vital functions. It’s widely used for prostate, kidney, and bladder cancers.
Follow-up is usually scheduled every 3–6 months in the first year and annually thereafter, depending on the type and stage of cancer.